



Nurse Mary used to spend four hours every weekend hunched over stacks of paper, manually correcting data errors before her Monday morning reports were due. As a senior SRHR provider at Chainda Urban Clinic in Lusaka, the high volume of clients meant that even small daily documentation errors could accumulate into major discrepancies by month’s end.
“I felt like I was working for the data, instead of the data working for me,” Mary recalls. “We were so busy serving women that the paperwork became a crisis we dealt with only when it was time to report.” — Nurse Mary, Chainda MCH
Across WISH 2 countries, one lesson has become increasingly clear: quality SRHR services depend on quality data. However, the pathways to improving data accuracy differ significantly depending on context. In Zambia, Ethiopia, and Madagascar, WISH 2 supported three distinct yet complementary approaches, each tailored to local realities, demonstrating how data systems can be strengthened from the clinic level to national structures.
Zambia: Provider-Led Micro-Innovation at Facility Level
At Chainda Urban Clinic, the challenge was not a lack of commitment, but the pressure of service volume. Documentation was often postponed until month-end, errors accumulated, and data became a source of stress rather than a tool for care.
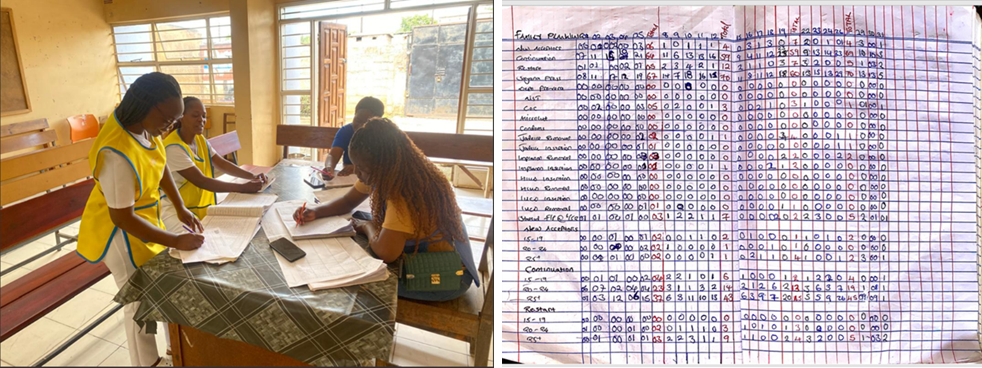
With WISH 2 acting as an enabler rather than an enforcer, Nurse Mary introduced a simple innovation: a Daily Summary Ledger, a hard-cover notebook used to reconcile service data at the end of each shift. This shifted data verification from a 30-day crisis into a 15-minute daily routine. Errors were identified and corrected immediately, creating a real-time feedback loop between service delivery and reporting.
The results were immediate and measurable. The clinic achieved a 100% match between facility registers and DHIS2, reducing data error rates from 15% in Q2 to 0% in Q3. Improved data accuracy strengthened supply chain forecasting, preventing contraceptive stock-outs and ensuring women received their preferred method. With no additional cost, the clinic freed 48 hours of health-worker time per month, which was reinvested directly into patient care.
Ethiopia: Rebuilding Systems in Fragile and Post-Conflict Settings
In contrast, the Afar Region of Ethiopia presented a fragile, post-conflict context where data challenges were systemic rather than procedural. Weak institutional foundations, inconsistent use of tally sheets, limited application of data quality assurance tools, skills gaps, and minimal data use for decision-making undermined service planning, particularly in pastoralist and conflict-affected communities.
Under WISH 2, FGAE and government partners implemented a comprehensive system-strengthening approach anchored in national and sub-national structures. This included training 29 data management providers across 14 facilities, institutionalising monthly Lot Quality Assurance Sampling (LQAS), establishing performance monitoring teams, and providing standardised HMIS and DHIS2 tools. Crucially, responsibility for data management was formally transferred to woreda and city Health Information Technicians, reinforcing government ownership and sustainability.
Technical oversight and verification were jointly conducted by sub-national health offices, FGAE Area Offices, FGAE Headquarters, IPPF, and third-party evaluators, OPM, supported by quarterly data verification, monthly reviews, and structured feedback loops. As a result, data completeness, accuracy, and timeliness improved significantly, and facilities increasingly used data to inform service planning and resource allocation. As noted by regional stakeholders:
“Supported health facilities have shown marked improvements in their data management systems, evidenced by more complete, accurate, and timely reporting, as observed during joint supportive supervision and routine data verification sessions with regional and sub-national health authorities.”
— Afar Regional Health Bureau HMIS Focal Person and SRHR Expert
Madagascar: Sustaining Change Through Government-Led Supervision
Unlike Zambia’s provider-led micro-innovation or Ethiopia’s post-conflict system rebuilding, Madagascar’s challenge lay in routine supervision and consistent government follow-through. Early assessments revealed that over 40% of facilities had discrepancies between registers and Monthly Activity Reports.
Rather than relying on one-off training, WISH 2 embedded data quality improvement within routine supportive supervision, led by Ministry of Health District and Regional teams. Supervision visits systematically compared reports against source documents, combined with on-the-job coaching and planned data cleaning. This hands-on, government-led approach reduced discrepancies, improved reporting timeliness, and strengthened provider confidence.

As observed by the Ministry of Health:
“During the Routine Data Quality Assessment supervision conducted with the WISH 2 team, we observed significant improvement in data use among health workers who received training on data analysis and utilisation. They adopted new ways of working, which contributed to better performance. Extending this capacity building to all health personnel would further strengthen the system.”
— Mr. Mamy Randrianasolo, Directorate of Family Health Data Manager, Ministry of Health
Service providers reported higher motivation, driven by constructive feedback and a clearer understanding of how accurate data supports programme performance and service improvement. Data quality shifted from a compliance requirement to a shared responsibility, reinforced by visible use of data for decision-making.
Together, these experiences demonstrate that there is no single solution to improving SRHR data quality. Zambia highlights the power of simple, provider-driven innovation; Ethiopia underscores the importance of institutional rebuilding in fragile environments; and Madagascar shows how routine, government-led supervision sustains improvement over time. What unites these approaches is WISH 2’s commitment to adaptive, context-responsive system strengthening, ensuring that accurate data ultimately serves its most important purpose: better SRHR care for women and girls.
Key Learning: Data quality improves when solutions are context-specific, embedded in routine systems, and owned by those closest to service delivery. Provider-led micro-innovations can rapidly improve accuracy at facility level; system rebuilding is essential in fragile settings; and government-led supervision sustains improvements at scale. Across all contexts, WISH 2’s adaptive approach—meeting systems where they are, strengthening ownership, and integrating data use into daily practice—proved critical to lasting change.

when
country
Zambia, Ethiopia, Madagascar
region
Africa
Subject
Media
Related Member Association
Family Guidance Association of Ethiopia, Fianakaviana Sambatra - Madagascar Association, Planned Parenthood Association of Zambia



